#neurodevelopmental
Text
sometimes i feel like people forget autism is a disability. and that’s not a bad thing! i’m all for disability acceptance, im proud of my disabilities. but i feel like we forget autism can hurt.
it hurts that i have to put more time and energy into socializing than others.
it hurts when i need to move so bad, usually cause im overwhelmed by either my surroundings or emotions, that i thrash and hurt myself.
it hurts that i cant be in places that are too loud or too bright, which on bad days can be as simple as a small, quiet noise or dim lights.
it hurts that i struggle to tell when im hungry, thirsty, tired, etc. so i can’t properly take care of myself. it doesn’t help my insomnia and i get very nauseas and get UTIs.
i 100% believe in autism acceptance. i don’t want a cure. but i also want us the acknowledge that it can hurt. it doesn’t mean my entire life will hurt, but some parts will. and i want a community where we can see both sides, see the hurt, and celebrate it anyway.
#autism#autistic#actually autistic#actually autism#autism acceptance#autism acceptence month#autistic things#autistic experiences#autistic community#autistic spectrum#autism spectrum disorder#autism spectrum#disabled#disability#disability pride#disabled pride#disabilties#autistic life#autism life#autism advocacy#neurodivergent#actually neurodiverse#neurodiversity#neurodevelopmental#developmental disabilities#developmental disability
15K notes
·
View notes
Text
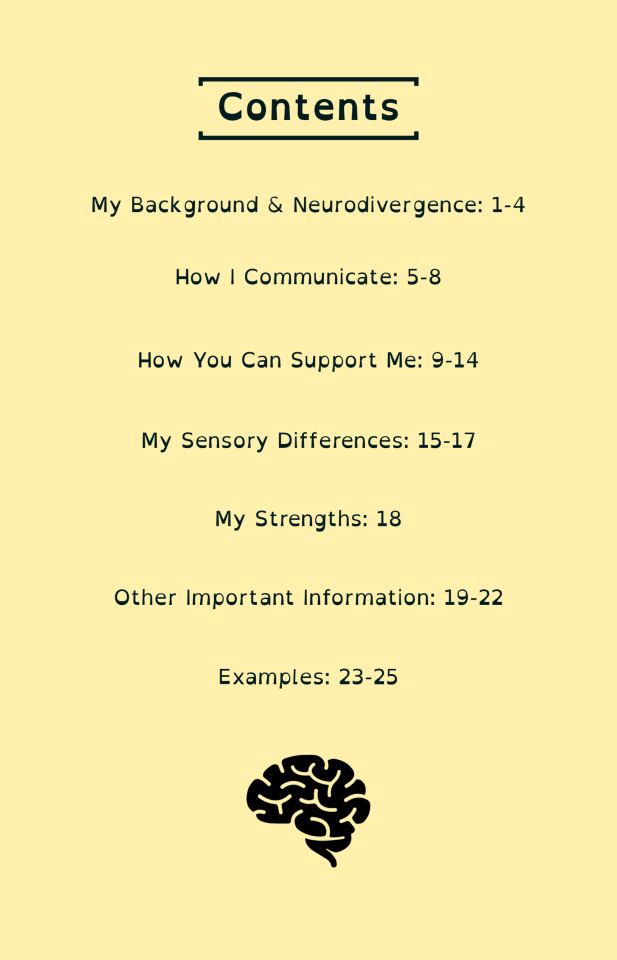
Neurodivergent Passport
A wee update with some exciting news about My Neurodivergent Passport: a tool to communicate your needs, strengths, and sensory/communication profiles.
Following some feedback the passport has been updated.
You can now get a printed version of My Neurodivergent Passport! You can buy it here!
You can also get it as a free PDF on my blog.

#neurodiversity#neurodiverse stuff#neurodivergent#neurodivergence#actually autistic#actually audhd#autism#audhd#adhd#dyspraxia#disability#disabilties#neurodevelopmental#intellectual disability#communication disorder#stuttering#asd#motor disorders#dcd#actually dyspraxic#dyspraxic#tics#tourettes#splds#dyslexia#dyscalculia#dysgraphia#fasd
3K notes
·
View notes
Text
Guys, lets talk in nice tone. Because momo genuinely want all to understand.
It no matter if you "consider self" disabled or not by autism. Autism is ASD, autism spectrum DISORDER. Aka, a neurodevelopmental disorder/disability.
Maybe not have ID/LD, maybe not be HSN or even MSN but if autism, than disabled.
If not disabled by symptoms then not autistic. IS LITERALLY IN DSM5........
Is ok if disagree but need know the actual facts that DSM5 only consider one autism if one is affected and disable by one autism. Just like all other neurodivergencies.
#disabled#actually autistic#actually disabled#autism#autistic#neurodivergent#autistic things#actually neurodivergent#neurodevelopmental#autistic thoughts#autistic community#autism community
304 notes
·
View notes
Text
It's annoying that ADD has not been a diagnosis since 1987 (or 2013 depending on how you define "not a diagnosis" as well as your source, either way at least a decade) and yet there are STILL people fighting tooth and nail to argue that ADD is it's own thing, or a thing at all.
It's ADHD-I. There is literally no difference between "ADD" and ADHD. They're the same disorder. It's just a subtype. The inattentive subtype. It's such a basic piece of misinfo yet it's EVERYWHERE.
#'but i was diagnosed with add!'#to that i say 'you shouldnt have been'#literally it helps noone to try and separate them#adhd#actually adhd#neurodivergent#actually neurodivergent#neurodiversity#neurodiverse#neurodevelopmental#mental health#disability#add#attention deficit hyperactivity disorder#attention deficit disorder#adhd issues#adhd inattentive#misinformation
714 notes
·
View notes
Text

I never see enough about the good things I experience because of Autism. Autism helps me hyper focus on things, makes me a more honest person and gives me amazing attention to detail! Yes it's hard at times but I love these things.
#actually neurodiverse#aspergers#autism#autism comic#neurodevelopmental#neurodivergent#neurodiversity#actually autistic#autism postitives
45 notes
·
View notes
Text
Am I stupid? Like genuinely? Because I thought I was smart because I used to be in advanced reading classes and stuff, but I don't think I am anymore.
I struggle with reading and writing a lot of the time.
I only know how to add, subtract, multiply, and divide and not very good at that, even with small numbers.
Bad at science concepts.
Only know special interest history stuff, and even get that stuff mixed up.
Talk 'like a toddler' most of the time.
Spend like 5 minutes on every sentence type online(less on this cause brain feels extra cotton-y, but still lots time).
Don't know names of symbols except period and comma.
Etc.
Is this autism regression or something else?
Don't want to lose writing skills more. I'm an author. Only way to make money. Need to survive.
Family not safe, no carer, no money for carer. Can't college, can't work, can't get diagnosis.
This impossible.
(Maybe have learning disability, no know)
#autism#actually autistic#developmentally disabled#neurodivergent#neurodevelopmental#neurological disability#disabled#disability#autism regression
29 notes
·
View notes
Text
What is oppositional defiant tic or oppositional tic?
This term is coined by Jess Thom aka Touretteshero. She has Tourette’s and is a public speaker and advocate on Tourette’s. She has a blog dedicated to sharing information and personal experiences. (This link will directly take you to her sharing her experiences with ODT)
Oppositional tic is a tic that makes you say, do, or think of something you’d normally wouldn’t do or never would do.
E.g.
Ticcing a Christmas gift secret in front of the person
Tics forcing you to tense your stomach muscles until you pee (bladder tic)
Gagging tic that could lead to a vomiting tic
Ticcing insults or rude comments when you’re the type of person that keeps negative thoughts and opinions to yourself
Ticcing slurs
Tics mimicking regular conversations and makes it seem like you’re directly speaking to someone, when you're not meaning to or are shy and would less likely strike up a conversation (e.g. ticcing questions, ticcing specific words or paragraphs like: “Cool shoes!” “Hello!” may be combined with waving, “How’s your day?” Etc.)
Suggesting or requesting the ticcer to stay silent in certain places (library, movie theater, etc.), not to do something in the building (e.g. A sign says not to tap on the glass after hearing or reading the sign the ticcer may immediately tap on the glass as a tic, etc.), giving an assignment not to drop or spill something the ticcer may end up breaking or spilling it.
Getting a mental picture (spilling food and drinks, throwing stuff, hitting someone or something), words or phrases (these will not lead to anxious behavior or OCD as tics are exclusively a tic disorder neurotype, if one has a anxiety disorder or OCD, mental tics can trigger anxiety and OCD)
What makes it an oppositional tic if the disorder is oppositional itself?
Oppositional tics includes more range of complex tics and not just inappropriate and slur tics. It shows and open up minds that tics can mimic everything the human body possibly can do.
Are coprophenomena terms problematic?
No, though it caused uneducated people to create / use the ablest term “the swearing disease / disorder”. It also has lead people to believe it's something we want to do or choosing to do to get away with it, which can be really difficult to talk about tics including mental tics.
Coprophenomena terms are perfectly okay to use. Coprophenomena only focuses on insults, slurs and inappropriate vocal, motor and mental tics, while oppositional tics focuses on more range of complex tics.
ODT / OT also focuses more on the ticcers experience with their inappropriate tics, instead of focusing on how society is distressed by it.
Here's a video of a tourettic womon who talks about OT / ODT
Snapple and Cats! - Oppositional Tics on youtube
#actually tourettic#tourette#tourette’s#tourettic#tourette syndrome#tic disorder#actually neurodiverse#neurodevelopmental#neurodivergent#neurodiversity#oppositional defiant tic#oppositional defiant tics#coprolalia#coprophenomena#oppositional tic#oppositional tics
11 notes
·
View notes
Text
Hitting developmental milestones unusually early is just as much a sign of a neurodevelopmental condition (i.e. autism, ADHD, learning disability, etc.) as hitting them late.
Doubly so if you hit some unusually early and others unusually late
16 notes
·
View notes
Note
Hi! Feel free not to answer this if im overstepping or it's inappropriate, but u made posts about neurodivergence and disability and you seem knowledgeable so I thought it would not hurt to ask. I have this friend with a neurodevelopmental disability and I don't know how to set boundaries with her? I understand she does not pick up the social cues I usually use with neurotypical people, but I don't want to be blunt and rude either. What is a way to tell her for example if I am having a conversation with someone else and want her to leave without saying it mean? If it was a neurotypical I could do body language or subtle hints but anything more than that feels rude to me. Thank you for reading and I hope you have a good day
Before start please remember just giving best advice possible and might not be much help since need others help set boundaries unless already in place.
Thing first important thing is to remember that when it comes to setting boundaries, you can’t really avoid sounding blunt or rude. Can remind person during talk that isn’t mad or trying be rude, might also help explain before talk begins.
Type of disability and severity can play role. Ask make sure even know what boundaries are, and not saying be rude, saying because broke so many not understanding what they are and how work. If don’t understand boundaries, explain what are, how work and why needed.
Would recommend that staying direct in setting boundaries. Say exactly what mean and want person understand. If mean one thing, don’t say another. Many neuredevelopmental people can’t see “in between the lines” and need it be said clearly.
Not everyone can grasp concepts of boundaries especially if high/higher support needs. If have carers, talk to them about helping explain what your boundaries are and how person can respect them. Also remember that might not get correct first time, doesn’t mean stop trying set boundaries, just mean need keep reminding and hep understand. If take a couple times before can remember or actually understand how boundaries work, don’t get mad at person. Just reexplain boundary that was broken and if possible (and helps person) act out scenarios where boundary is broken and met.
Hope helps and ask if any more questions
8 notes
·
View notes
Text
im autistic and have albinism / am albino ❌
assigned AA battery at birth ✔️
#ive had a realization#yeah for those who dont know i have albinism!#you may reblog even if doesnt apply to you btw!#disabled#disability#albino#albinism#autism#autistic#neurodevelopmental#neurodivergent#actually autistic#actually neurodivergent#genetic condition#skin condition#actually albino
123 notes
·
View notes
Text
How Common is Neurodivergence?

[image id: poster of "How Common is Neurodivergence?.” There are 12 circles and five small images: an image of a brain, speech bubbles, an infinity sign, a person reading, and a person surrounded by arrows and balls. Each of the 12 circles has a percentage representing how common a particular form of neurodivergence is written in Open Dyslexic font. Full transcript, more information, and references under the cut.]
More Information
Forms of neurodivergence represented here are focused on neurodevelopmental disorders.
These percentages are representative of percentage in general population and do not reflect percentages within neurotypes which are often higher due to co-occurrence being the norm, rather than the exception, within neurodevelopmental disorders; for example, 33-45% of people with ADHD will also have dyslexia (Butterworth & Kovas, 2013), whereas only 10% of the general population are dyslexic (British Dyslexia Association [BDA], 2023).
Certain neurodivergencies are often underrepresented and under-reported, so the percentages are likely to be higher; for example, one study suggests that rates for FASD in the UK may be as high as 17% (McQuire et al., 2019).
Some of the neurodivergencies represented here are umbrella terms and percentages given are representative of all forms of neurodiversity belonging to that term; for example, SpLds include dyslexia which is at a rate of 10% (BDA, 2023) and dyscalculia which is at 3-7% (Haberstroh & Schulte-Körne., 2019). Tic Disorders at 1% are another example here, as this is inclusive of Tourette Syndrome which is at 0.6%, and around 1 in 5 individuals exhibit tics at some point during childhood (Cavanna et al., 2017).
______________
Transcript in Full
1% Intellectual Disability
10% Language Disorder
4% Speech Sound Disorder
5% Stuttering
7.5% Social (Pragmatic) Communication Disorder
1.7% Autism
5% ADHD
10% Specific Learning Disorder (SpLD)
5% Developmental Co-Ordination Disorder (DCD)
3-4% Stereotypic Movement Disorder
1% Tic Disorders
3.6% Fetal Alcohol Spectrum Disorders (FASD)
______________
Sources
American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders (5th Ed., Text Rev.).
Arvidsson, O., Gillberg, C., Lichtenstein, P., & Lundström, S. (2018). Secular changes in the symptom level of clinically diagnosed autism. Journal of Child Psychology and Psychiatry, 59(7), 744–751.
Attention-deficit/hyperactivity disorder (ADHD). PsychDB. (2022, November 29).
Autism spectrum disorder (ASD). PsychDB. (2022, May 19).
Butterworth, B., & Kovas, Y. (2013). Understanding neurocognitive developmental disorders can improve education for all. Science, 340(6130), 300–305.
Cavanna, A. E., Coffman, K.A., Cowley, H., Fahn, S., Franklin, M. E., Gilbert, D.L., Hershey, T.G., Jankovic, J., Jones, M., Leckman, J.F., Lehman, R., Mathews, C.A., Malaty, I., McNaught, K., Mink, J.W., Okun, M.S., Rowe, J.A., Scahill, L.D., Scharf, J.M., Schlaggar, B.L., Stewart, E., Walkup, J.T., Woods, D.W.. (2017). The spectrum of Tourette Syndrome and TIC disorders: A consensus by Scientific Advisors of the Tourette Association of America. Tourette Association of America.
British Dyslexia Association. (2023). Dyslexia. British Dyslexia Association.
Dyspraxia at a glance. Dyspraxia Foundation. (2023).
Haberstroh, S., & Schulte-Körne, G. (2019). The Diagnosis and Treatment of Dyscalculia. Deutsches Arzteblatt International, 116(7), 107–114.
Ketelaars, M. P., Cuperus, J. M., van Daal, J., Jansonius, K., & Verhoeven, L. (2009). Screening for pragmatic language impairment: The potential of the Children’s Communication Checklist. Research in Developmental Disabilities, 30(5), 952–960.
May, P. A., Baete, A., Russo, J., Elliott, A. J., Blankenship, J., Kalberg, W. O., Buckley, D., Brooks, M., Hasken, J., Abdul-Rahman, O., Adam, M. P., Robinson, L. K., Manning, M., & Hoyme, H. E. (2014). Prevalence and characteristics of fetal alcohol spectrum disorders. Pediatrics, 134(5), 855–866.
McQuire, C., Mukherjee, R., Hurt, L., Higgins, A., Greene, G., Farewell, D., Kemp, A., & Paranjothy, S. (2019). Screening prevalence of fetal alcohol spectrum disorders in a region of the United Kingdom: A population-based birth-cohort study. Preventive Medicine, 118, 344–351.
Norbury, C. F., Gooch, D., Wray, C., Baird, G., Charman, T., Simonoff, E., Vamvakas, G., & Pickles, A. (2016). The impact of nonverbal ability on prevalence and clinical presentation of language disorder: Evidence from a population study. Journal of Child Psychology and Psychiatry, 57(11), 1247–1257.
Polanczyk, G. V., Willcutt, E. G., Salum, G. A., Kieling, C., & Rohde, L. A. (2014). ADHD prevalence estimates across three decades: an updated systematic review and meta-regression analysis. International Journal of Epidemiology, 43(2), 434–442.
Polanczyk, G., de Lima, M. S., Horta, B. L., Biederman, J., & Rohde, L. A. (2007). The worldwide prevalence of ADHD: A systematic review and metaregression analysis. American Journal of Psychiatry, 164(6), 942–948.
Prevalence and Therapy Rates for Stuttering, Cluttering, and Developmental Disorders of Speech and Language: Evaluation of German Health Insurance Data. (2021). Frontiers in Human Neuroscience, 15(645292), 1–13.
Social (pragmatic) communication disorder. PsychDB. (2021, March 29).
Stereotypic movement disorder. United Brain Association. (2022, August 8).
Wren, Y., Miller, L. L., Peters, T. J., Emond, A., & Roulstone, S. (2016). Prevalence and predictors of persistent speech sound disorder at eight years old: Findings from a population cohort study. Journal of Speech, Language, and Hearing Research, 59(4), 647–673.
UCL. (2013, April 19). Learning disabilities affect up to 10 per cent of children. UCL News.
#neurodiversity#neurodiverse stuff#neurodivergent#neurodivergence#actually autistic#actually audhd#autism#audhd#adhd#dyspraxia#disability#disabilties#neurodevelopmental#intellectual disability#communication disorder#stuttering#asd#motor disorders#dcd#actually dyspraxic#dyspraxic#tics#tourettes#splds#dyslexia#dyscalculia#dysgraphia#fasd
358 notes
·
View notes
Text
There is some discourse on Twitter about zayn possibly being autistic. Zayn is neurodivergent and was diagnosed with adhd when he was younger. I'm not certain he has autism as well. However, it wouldn't be a far-fetched idea considering that people with adhd are usually comorbid with autism. With that being said, a lot of people forget that adhd has similar traits as autism ex. Stimming, trouble socializing, anxiety comorbidities, emotional dysregulation etc. adhd isn't just some "behavioral" defect that makes you hyperactive, it's literally a neurodevelmental disorder. So, no I'm not exactly sure that zayn has autism, however, I can see how people would come to that conclusion.
#zayn#zayn malik#autism#adhd#neurodivergent#neurodevelopmental#one direction#liam payne#harry styles#louis tomlinson#niall horan
6 notes
·
View notes
Photo
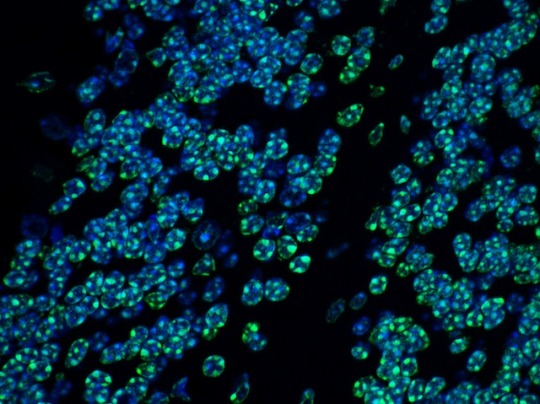
A Quiet Brain
Sometimes there’s so much running through our brain that we wish we could turn down the noise. At a molecular level, there are proteins doing just that. HUSH – the human silencing hub – is a collection of proteins that patrol our genes, keeping repetitive elements quiet when they’re not needed. MORC2 and MPP8 are two of these, and bind to bundles of DNA to silence genes (green in the mouse cerebellum pictured). Mutations in these proteins are linked to neurodevelopmental disorders. Researchers found the proteins at high concentrations in neurons, helping to regulate material that accumulates to give each neuron a unique identifying fingerprint. Without HUSH, neurons lost their identity, which makes it hard to make the right precise connections with other cells. Similar findings in human cells in the lab suggest the same thing happens in our brains, and that disruption to this regulation could be behind multiple mental disorders.
Written by Anthony Lewis
Image from work by Astrid Hagelkruys and colleagues
Institute of Molecular Biotechnology of the Austrian Academy of Sciences (IMBA), Vienna, Austria
Image copyright held by the original authors
Research published in Science Advances, November 2022
You can also follow BPoD on Instagram, Twitter and Facebook
52 notes
·
View notes
Text
“I am a chad texture enjoyer” -me, 2023
5 notes
·
View notes
Text

When you receive a diagnosis...
The questions that come with this are nearly as many as they were before. I found myself going back over my entire life trying to work out what was Autism and what was me for many years. I finally worked out its all me, Autism is just one part of me.
#autism comic#autism#aspergers#actually neurodiverse#neurodivergent#neurodiversity#neurodevelopmental
18 notes
·
View notes
Text
Autism and ADHD Coaching
Hello,
I wanted to reach out to the Tumblr ADHD and/or Autism community to let you know I am offering Neurodiversity coaching for adults. I am offering virtual meetings, with short initial meetings to see if we are a good fit and if you think continuing the sessions would be interesting or helpful for you.
First session = 30min session for $15
The $15 will be asked at the end of the consultation, contingent on your satisfaction.
If you wish to continue to more sessions we can discuss timing that you feel fit your specific needs. In general, my rate will be $30 for 1 hour sessions.
So, if you are interested in:
getting guidance on whether you might have ADHD or Autism, and if you are interested in pursuing an official diagnosis, what that can mean and how to go about it through official channels
learning ways to work WITH your brain instead of against it
just want someone to listen who understands what it's like to be neurodivergent in a neurotypical world
show you new ways of looking at mental health
help you identify your gifts and talents
Please text me at 215-450-5814 if you have additional questions or to set up a session time!
Or please visit my website at brainhacking.org
Things of note:
I am not an official doctor or a liscense, I CAN NOT give you any official diagnosis or access to medication
I am neurodiverse myself (both Autism and ADHD) and while I was assigned female at birth I consider myself agender
I am a scientist and have a degree in Neuroscience with specialties in Neurodevelopment and Psychiatry
I believe strongly in improving quality of life and not cure research
I am an expert in neurodiversity and do a lot of neuroadvocacy work to the point I am considering achieving the degrees needed to make this kind of coaching official
I am currently working on creation of new scales that address ACTUAL symptoms of ADHD/ASD/C-PTSD instead of the white male child in a classroom focus they have in the DSM. I excel in AFAB symptoms or atypical male symptom presentation.
Something of additional note.... I have 2 friendly cats, one of which is a 4-month old kitten and both are likely to cameo during calls.
Mentioning this for no particular reason ;)
#neurodivergent#neurodiversity#ADHD#ASD#Autism#mental health#depression#anxiety#PTSD#C-PTSD#Queer#Gay#anime#coaching#neurodevelopmental#psychology#psychiatry#ADD#attention#lesbian#cat#cats#kitten#kittens#baby animals#comfort#therapy#warmth#peace#accessibility
3 notes
·
View notes
Last Seen Blogs

spookedwhorse
yea, well; you know

unhappyhipsters
Unhappy Hipsters

elle-cz
Elle

workingmoms911-blog
Working Moms 911

arganga
Untitled