#queer theory
Text
Cis people getting trans surgeries doesn't scare me at all. I've seen cis girls who got top surgery for body mod reasons and they look cool as hell. I've seen ace people whose gotten bottom surgeries because they want to be less capable of sex. It's cool and normal actually.
#196#my thougts#leftist#leftism#top surgery#bottom surgery#trans#transgender#transmasc#transfem#queer rights#queer theory#queer
5K notes
·
View notes
Text
aspec terms for beginners!
since it's trending right now, i feel like it might be helpful to clear up some basic aspec (but particularly aromantic, as we are the center of attention currently) terms. if you have absolutely any questions, i would be happy to answer, either in the replies, dms, or my inbox!
★・・・・・・★
the split attraction model (SAM): a model of human behavior that posits that, for some people, romantic and sexual attraction are not the same.
[most often this will come in the form of someone being aspec on one axis and allo (not aspec) on another. for example, a biromantic asexual may be romantically attracted to two or more genders, but sexually attracted to none. some people may even use SAM for allo identities– a bisexual lesbian may be sexually attracted to multiple genders, but only romantically attracted to women (note that this is not the only way that someone can be an mspec lesbian, just one way!). the SAM does not apply to everybody, not even all aspecs! there are non-SAM aros, for instance, who do not differentiate their aromanticism from their sexuality.]
aspec: a collection of queer spectrums centered around the lack of a certain attraction or identity. the most common spectrums under the aspec umbrella are asexual, aromantic, agender, and aplatonic, though there are many other ways to be aspec.
asexual: experiencing little to no sexual attraction.
[aces can still have sex– whether its because they experience some amount of sexual attraction or they just want to participate in sex because they find the act appealing in some other way. that being said, there are still plenty of aces who have not and will never have sex. it is a spectrum.]
aromantic: experiencing little to no romantic attraction.
[aros can still have romantic partners– whether its because they experience some amount of romantic attraction or they just find relationships appealing in some other way. that being said, there are still plenty of aros who have not and will never be in a romantic relationship. it is a spectrum.]
agender: having no gender or little relation to any gender.
aplatonic: experiencing little to no platonic attraction.
[similarly to aros and aces, apls can still form friendships if they so desire– whether its because they experience some amount of platonic attraction or they find friendships appealing in some other way.]
aroallo: combination of aromantic and allosexual– allosexual being someone who fully experiences sexual attraction. an aroallo, then, is someone who is aromantic but not asexual. aroallos often do not have a standard relationship with sex due to its romantic connotations and the stigma against loveless sex. someone having sex with someone else they do not love does not inherently make them aroallo, much in the same way that having a nonsexual relationship with a partner doesn't inherently make either participant asexual.
aroace: someone who is both aromantic and asexual. because aro and ace are both spectrums, an aroace may still experience some amount of attraction on either or both of those spectrums, or they may experience attraction of some other kind (platonic, tertiary, etc.), and that attraction may be only for a certain gender or genders– these are known as oriented aroaces.
queerplatonic relationship: a type of relationship that is defined only by the people within it. i have a post dedicated to explaining this in larger detail.
partnering: an aspec (usually aromantic) person who has and/or desires to have a partnership or multiple partnerships– romantic, queerplatonic, or otherwise.
non-partnering: an aspec (usually aromantic) person who has no desire to form a partnership of any kind.
romance/sex/plato favorable: an aspec who desires or would not reject a romantic, sexual, or platonic relationship. they are also generally not particularly bothered by seeing these relationships in their day-to-day.
romance/sex/plato repulsed: an aspec who does not desire a romantic, sexual, or platonic relationship and generally does not like seeing those relationships in their day-to-day. [x] repulsed people are not necessarily judgemental towards people who desire or participate in those relationships, they just do not desire them for themselves. repulsion often takes the form of discomfort or annoyance. [x] repulsed people are not necessarily cruel sticks-in-the-mud– they are perfectly capable of being respectful, and they very often are. repulsion does not always stem from trauma, though it certainly can.
romance/sex/plato positive: not to be confused with favorability, [x] positivity is the belief that romance, sex, and platonic relationships are human rights that should be supported and uplifted. someone can be [x] repulsed and [x] positive at the same time, because favorability/repulsion revolves around the self, and positivity/negativity extends to others.
sex/romance/plato negative: not to be confused with repulsion, [x] negativity is an inherently judgemental and harmful ideology. most commonly in the form of sex negativity, these ideologies are centered around the opposition to or personal judgement of people who engage in romance, sex, or platonic relationships. sex negativity in particular is embedded in western white supremacist societies and it is important for aspecs not to play into that.
those are the basics, but i have more information below the cut!
★・・・・・・★
> how are aspecs queer?
aspecs are queer because "queer" does not only mean LGBT. queer theory is about far more than just LGBT people– though they are undeniably a large part of it– queerness is any subversion of the traditional cisheteronormative standard. this includes things that cishets may take part in/identify with, because you do not have to be LGBT to subvert those standards. cishets who are gender-nonconforming are queer, for example. a good rule of thumb is that if you have to explain what you whole deal is to cishets, you're queer. queer does mean strange, after all.
traditional cisheteronormative conceptions of attraction, gender, and relationships do not account for aspecs. it is expected that everyone will one day form a traditional partnership with one other person, and that relationship will include sex (even if only for procreation, under some dogmas). virginity past a certain age is seen as a point of shame and something indicative of a larger problem in someone– in men, a red flag even. people past 30 without a relationship are pitied. our economic structure is build for couples and families– it's near impossible for someone to live comfortably alone. romance, friendship, and love are placed on a pedestal, treated as the meaning of life, the best thing anyone could ever experience. "love is the point of everything," as many posts on this site like to claim. people who reject these ideas are undeniably queer.
> i can get behind aros and aces, but the whole "aplatonic" thing feels like a stretch to me. how is not having friends queer? "platonic attraction" isn't even real.
aplatonicism is more than just "not having friends," and many apls have friends anyway, much in the same way that aros can date and aces can have sex. someone who does not have friends is not inherently aplatonic, they only are if they identify that little-to-no platonic attraction in themselves and choose to label themselves that way (just like how virgins aren't inherently asexual). still, apls who don't have friends exist, and they are all queer. what is a greater subversion of traditional cisheteronormative relationship structures than an outright rejection of what's seen as the most basic, fundamental relationship our culture has to offer?
you may not feel that platonic attraction is a distinct phenomenon in your own experience, and that's fine! ultimately, a lot of aspec terms exist for the utility and comfort of aspecs themselves. the SAM isn't for everyone, and platonic attraction isn't for everyone either. you do not have the authority to tell people what their own experiences are, nor should you care.
> i think it's sad that you're limiting yourself with these labels. you'll find someone one day!
for the broad majority of aspecs, our identities are not self-disciplinary, nor are they necessarily permanent. all queer people are capable of misunderstanding their identity or having a fluid identity– it is not a problem unique to being aspec. that being said, a lot of us may always be aspec and completely happy with it. being aspec is not a tragedy. the only thing i don't like about being aromantic is the judgement i receive from other people about it. non-partnering aspecs are not "missing out" on anything, because we don't even want the things we're rejecting in the first place. many of us are romance/sex/plato repulsed and are far more happy engaging with the world and with other people in different ways, because there is so, so much more to life than relationships, and it's wrong to presume that relationships are universally fit for everybody. telling an aspec that they'll find "the right person" one day is no different from telling a lesbian she'll find "the right man" one day. there is no "right person" for an aspec just as there's no "right man" for a lesbian. a lesbian is not "missing out" on a heterosexual relationship just because it's culturally perceived as superior and more fulfilling.
[disclaimer before anyone tries to do a "gotcha," i'm talking about a lesbian who is fully not attracted to men in any way. it's not like homophobes know the intricacies of gender identity and nonconformity as it pertains to homosexuality anyways.]
lastly, i wanna give a special shout out to the loveless aros and the relationship anarchists.
loveless aros are those who either feel little-to-no love as they understand it, or they are someone who supports the de-centering of love. they're worthy of a whole post of their own, but in summary: the loveless experience is all about finding joy in yourself and the countless things our world has to offer that are not dependent on the vague idea of love.
relationship anarchy is another concept worthy of its own post, but in essence it's an ideology aimed at abolishing the standard hierarchy of relationships (in the USA, depending on who you ask, its typically friendship < family < romantic partnership or friendship < romantic partnership < family) and allowing everyone the autonomy to define their relationships for themselves.
if i made any mistakes, let me know! and of course i'm willing to answer any questions anyone may have. :-3 thanks for reading my long ass post!
#barking#aromantic#aspec#romance repulsed#aroallo#aplatonic#asexual#aroace#loveless#queer#lgbt#queerplatonic#alloace#queer theory#relationship anarchy#split attraction model#aro#ace#apl#agender#long post
2K notes
·
View notes
Text




Deeply important. When purity-consciousness overwhelms a movement, it often ends up doing its enemies work for it.
Direct link to thread below, above images screenshotted for posterity:
#queer theory#lgbtqia#if you want to tag this q-slur you need to understand you may be complicit in this quite bluntly#every word for the non normative ends up as a slur#queer#queer as in fuck you
27K notes
·
View notes
Text
i understand wanting to share how much you always hated everything somerton has ever said, really i do, but you guys. a lot of the work he plagarized is, actually, you know. good. some of it is seminal queer theory. you don't have to agree with everything, but it's worth engaging with those writers/creators' work directly before dismissing it outright because you were introduced to it through the shitty lense of a james somerton video.
#og#james somerton#hbomberguy#plagarism#the celluloid closet#queer theory#queer studies#hbomber literally made a playlist of youtubers somerton directly stole from so you can check out their stuff
1K notes
·
View notes
Text
I am Sage's mother, better known as Nana. I adopted Sage after my son died when she was still a baby. She's been through six foster homes by then, but we loved her and she blossomed into a joyful, lively girl who made music and art.
Puberty began and COVID hit, and she was treated for depression and anxiety, at times very severe. Her teachers shared any concerns with me so her treatment could be adapted.
The transparency ended in August of 2021 when Sage started high school. She started a public high school and she told me that all the girls there were bi, trans, lesbian, emo and she wanted to wear boy's clothes and be emo. Because I saw it as just a phase, it was fine with me.
But at school, she told them something different: she was now a boy named Draco with male pronouns. Sage asked the school not to tell me, and they did not tell me even though I informed them of her mental health history and medication. If I had known, this would be a much different story.
She was terribly bullied. No one told me. But boys followed her, touched her, threatened violence and rape. Something happened in the boy's bathroom but for two days, the school told me nothing. They kept meeting with Sage alone and she became so distraught they called me to pick her up.
That evening, I found a hallpass labeled 'Draco' and Sage told me she was identifying as a boy, and that her counselor said she could use the boy's bathroom. She'd been jacked up against the wall by a group of boys. She was crying, terrified. I said just stay home, we'll figure it out. That was my last conversation with Sage for five months.
The night she ran, she thought, to a young friend she'd met online, she left a note saying she was scared of what would happen if she stayed. The sheriff, FBI, search dogs were called in. I dropped to my knees in prayer. Nine days later the FBI found her in Baltimore. My baby had been lured online, sex trafficked by DC then Maryland. She was locked in a room, drugged, gang raped and brutalized by countless men. It was night. The FBI told us to pick her up in Maryland the next morning.
We packed our cars with blankets and stuffed animals and arrived by 8 am, but we were told we couldn't see her, and were summoned before Judge Robert Kershaw late that afternoon. They didn't even tell Sage that we came for her. We finally entered the courtroom and Sage appears on a huge Zoom screen from a prison cell. She looks tiny and broken, and I cry out 'I love you Sage.' Sage responds 'I love you too, Nana.' But attorney Anisa Khan rebukes us. She is a 'he' and his name is 'Draco' not Sage. We were floored.
Khan accuses us of emotional and physical abuse, that we are misgendering her, even though we just learned she claims to be trans and we're willing to use any name and pronouns to bring her home. My husband was so tearful he kept forgetting the new pronouns, so the judge had the bailiff remove him from the courtroom. I was pleading for my child to be returned and treated for her unspeakable trauma. Judge Kershaw told me, if I use the word 'trauma' again, he would throw me out too.
For over two months, he withheld custody. He housed Sage in the male quarters of a children's home. Sage told me she was the only girl and repeatedly assaulted. She was given street drugs by the other kids and Khan told her she didn't care. She just wanted to win the case and all the way to the Supreme Court if necessary. Khan tried to prove abuse, but we were eventually cleared by both states of all charges.
Sage later told me Khan had told her to lie that we hit her. Khan even had Sage's school counselors testify against us, though they barely knew Sage and they didn't know us at all. Khan told my precious child I didn't want her anymore. I found out Sage never received any of the letters I sent her.
Sage ran from the Children's Home and disappeared for months. They told me she might already be gone forever, but I couldn't give up and I finally found a tip on her social media that led the marshals to her in Texas. She had been drugged, raped, beaten and exploited. This time I was able to be with her for the traumatic rape exam, and to bring her home.
Back in Virginia, she entered the mental health facility that Judge Kershaw had ordered, as it would affirm her as a male. The therapist began pressuring her to have her healthy breasts removed. Sage was too scared to protest, but she asked me to secretly buy her girl's clothes because she wanted to be a girl, but keep them in the car. It took a kind lawyer, Josh Hetzler to secure her discharge.
After almost a year. Sage was finally home. Safe. Alive. Sage is receiving professional trauma care. The first trafficker has already been convicted. Sage has nightmares, panic attacks, rape-related medical issues, but there's hope. I tell her she's not broken she's just scarred. And part of that hope is that in courageously sharing her story, others will be saved.
Sage said she doesn't know who she was back then. She wasn't a boy, she just wanted to have friends. But her school, the judge, the attorney and the doctor were all blinded by their ideology. The consequences for Sage were unspeakable.
Please don't let ideology harm another child. Let parents do our jobs. We know our children best and we love them a million times more.
Thank you.
==
Jesus Christ. This girl was exploited by everybody, except for her parents, who were villainized for literally nothing. It's opposite world.
And the fact that everybody with authority prioritized stupid shit like pronouns and trying to coax her further down into a fake identity, even against her will, and other ideological bullshit over her actual wellbeing is disgraceful.
The judge and attorney need to be disbarred, the therapist stripped of their license, and everyone who conspired to separate Sage from her parents fired.
#Sage's Law#HB 2432#gender ideology#queer theory#ideological corruption#genderwang#safeguarding#child safeguarding#predators#groomers#predatory#gender cult#religion is a mental illness
2K notes
·
View notes
Text

#fight club#the narrator#tyler durden#guy hocquenghem#gilles deleuze#soapshipping#sigma male#male satire#gay#whispers#gaycel#mlm yearning#male manipulator#queer theory#theory fiction
346 notes
·
View notes
Text
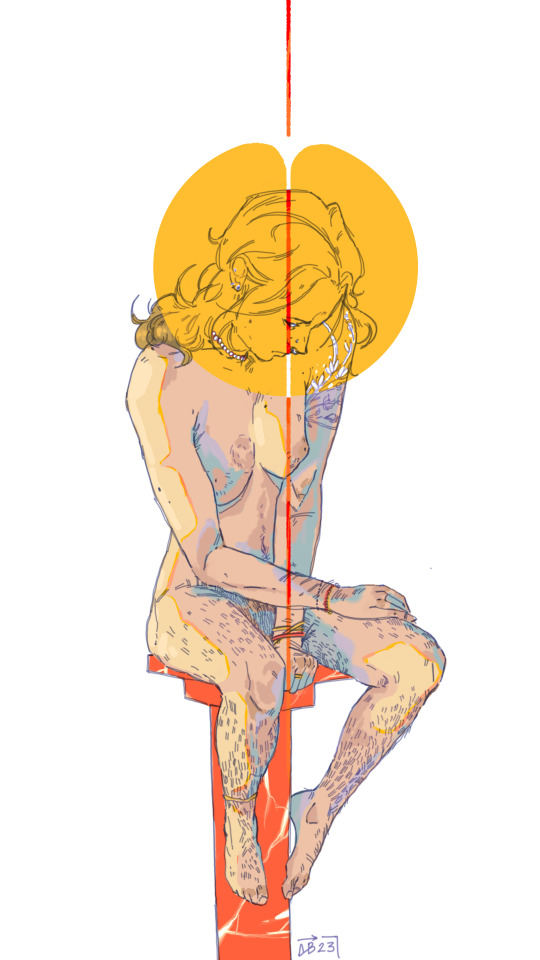
Something about my transsexualism...
[I.D.: Digital colored drawing of a white trans figure sitting slouched on a red marble column on a white background. They have a broken yellow circle around their head, split by a red and white line down the center of the image. The figure is wearing small bracelets, necklaces, and earrings. Their floral shoulder tattoo is colored in white. End I.D.]
#trans artwork#trans art#trans artist#cw nudity#queer theory#transmasc#trans#transgender#trans pride#ftm#trans men#transmasculine#trans masc#trans community#mtf#trans women#transfeminine#trans fem#transfeminism#queer joy#trans joy#queer#lgbt#pride#queer pride#you figure out the symbolism
2K notes
·
View notes
Text
queer theory is actually a nightmarish frankensteinian creation of postmodernism, and post-modernists philosophers have frequently and explicitly been pro-pedophilia, because this is a logical consequence of what post-modernism says is true: there is no (epistemic) certainty or stable meaning.
when my conservative parents tell me they basically associate "lgbtq" with "maps" and pedophilia, they have reason to do so, given how "queer culture" is fundamentally a creation of post-modernist values, and post-modernist estimations of sexuality. everything is fluid, no binary exists, no meaning is fixed, so there are no defining lines, which means lines cannot actually be crossed. homosexuals can be bisexual, man and woman are interchangeable meaningless terms, and attraction to children is just one of the many ways sexual fluidity is expressed in humans, a benign and normal thing that should be released from modernist moralistic confines
that is queer philosophy, and it is actual queer culture. so not only are LGB folk being told they should celebrate the reclamation of an awful slur that explicitly others them as "perverted" and "strange", but now they are told to embrace queer culture (which means queer identity and philosophy) which not only declares their reality as abnormal and unreal (same-sex attraction is myth, since there is no such thing as sex and attraction is fluid), but also defines them explicitly with sexual perversions like pedophilia and bdsm: which IS EXACTLY WHAT HOMOPHOBES BELIEVE ABOUT THEM.
when queer culture is predicated on subjective feelings of identity needing to be validated, celebrated and "set free" from modernist (read definable, material and epistemological) structures, then the distaste for MAPs from queer folk doesn't mean anything, because even if MAPs are publicly rejected by queer culture, they are embraced and validated by queer theory and post-modernist philosophy.
what is doubly baffling to me is how the lgbtq+ community has tainted a movement for gay rights, you know, people who are being killed and ostracized for being same-sex attracted. not only nullifying their experiences and struggle in being same-sex attracted, not only associating their neutral, normal orientations with perversions and kinks, making something neutral political . . .
but they have also actively decentered a movement for homosexuals and bisexuals in order to accommodate identities that have NOTHING to do with that struggle or fight. intersex conditions, gender dysphoria, and asexuality have nothing to do with the oppression LGBs have faced for their sexual orientation and gender nonconformity, their culture of genderlessness. the idea that men and women can wear and present however they want, love and be attracted to the same sex, without it altering their material status.
EVEN MORE INFURIATINGLY, queer politics has offered almost ZERO challenges to patriarchy. by throwing out definitions, throwing out distinctions, it has relegated the essence of oppression to an individualistic, liberal fantasy that is powerless to change the system, and so can only grant us "spicy" patriarchy. dominance and submission, patriarchal inventions, are now cool kinks that every couple should try. gender is now open access (but still necessary), so men can wear heels and still call women slurs and violently harass them. transmen can go by he/him and still be refused abortion access! gay people are gender fetishists, not sinners. nothing has structurally changed, it's just we have cool names now! :)
so now LGB and women all over the fucking world are relegated to this homophobic misogynistic hell whether we turn to the left or right, and when we speak up about it, conservative homophobes and misogynists confuse us with liberal perverts, and liberal homophobes and misogynists conflate us with conservative sadists.
the structure doesn't change. there is no actual progress. like, same-sex right and women's movements all over the world have suffered for this. because white liberal westerners wanted to play around with words and have that count as activism.
i fucking hate queer theory and politics. i fucking hate how rich western whites shit on every human rights movement while capitalizing on them.
462 notes
·
View notes
Text

Currently in Miami for a wedding, and I couldn't have survived the trip here without some books.
#dark academia#books#academic#dark academia aesthetic#dear diary#booklr#booktok#agatha christie#queer theory
188 notes
·
View notes
Text
Freindly reminder that you can't hate men without being queerphobic. You can't think men are inherently more dangerous, violent or sexual, or any of the other things people say about men without being inherently queerphobic.
You can't think these things about men without branding mlm as outsiders who will always be unwholesome and dangerous without women to "civilize" them.
You can't think these things about men without thinking of wlw who are more masculine as being inherently lesser for being like men.
You can't think these things about men without making most transfems seem suspect for having masculine traits, or forcing trans women to prove themselves female enough to be valid.
You can't think these things about men without telling transmascs that they are inherently degrading themselves by transitioning, or forcing them to deny their transition to be supported.
You can't think these things about men without basically calling all enbies female, and then calling all masc enbies dangerous.
You can't think these things about men without easing aspec men and/or calling their identities into question.
You can't think these things about men without basically telling intersex people they don't exist, and making intersex women feel lesser for having male traits.
If you hate men you will hate every letter in the LGBTQIA for having traits in common with men. Feminism that views men as the enemy will inevitably be Feminism only for cishet women.
#196#my thougts#queer rights#queer theory#feminism#mysandry#queer#lgbt#asexual#ace#aspec#enby#non binary#nonbinary#bisexaul#transmasc#transfem#trans#transgender#trans rights#transgirl#intersex#bi#mlm#wlw#gay#lesbian
3K notes
·
View notes
Text
By: Beth Bourne
Published: Feb 27, 2024
Kaiser gender specialists were eager to approve hormones and surgeries, which would all be covered by insurance as “medically necessary.”
On September 6, 2022, I received mail from my Kaiser Permanente Davis Ob-Gyn reminding me of a routine cervical screening. The language of the reminder stood out to me: “Recommended for people with a cervix ages 21 to 65.” When I asked my Ob-Gyn about this strange wording, she told me the wording was chosen to be “inclusive” of their “transgender” and “gender fluid” patients.
Based on this response, several thoughts occurred to me. Could I expose the medical scandal of “gender-affirming care” by saying and doing everything my daughter and other trans-identifying kids are taught to do? Would there be the type of medical safeguarding and differential diagnosis we would expect in other fields of medicine, or would I simply be allowed to self-diagnose and be offered the tools (i.e. hormones and surgeries) to choose my own gender adventure and become my true authentic self?
If I could demonstrate that anyone suffering from delusions of their sex, self-hatred, or identity issues could qualify for and easily obtain body-altering hormones and surgeries, all covered by insurance as “medically necessary” and potentially “life-saving” care, then maybe people would finally wake up. I certainly had.
I was prepared for failure. I wasn’t prepared for how easy success would be.
* * *
I am a 53-year-old mom from Davis, CA. My daughter began identifying as a transgender boy (social transition) and using he/him pronouns at school during 8th grade. Like several of her peers who also identified as trans at her school, my daughter was a gifted student and intellectually mature but socially immature. This shift coincided with her school’s sudden commitment to, and celebration of, a now widespread set of radical beliefs about the biology of sex and gender identity.
She “came out” as trans to her father (my ex-husband) and me through a standard coming-out letter, expressing her wish to start puberty blockers. She said she knew they were safe, citing information she had read from Planned Parenthood and the World Professional Association for Transgender Health (WPATH). To say I was shocked would be an understatement. I was also confused because this announcement was sudden and unexpected. While others quickly accepted and affirmed my daughter’s new identity, I was apprehensive and felt the need to learn more about what was going on.
Events began escalating quickly.
During a routine doctor’s visit scheduled for dizziness my daughter said that she was experiencing, the Kaiser pediatrician overheard her father using “he/him” pronouns for our daughter. The pediatrician seemed thrilled, quickly asking my daughter about her “preferred pronouns” and updating her medical records to denote that my daughter was now, in fact, my son. The pediatrician then recommended we consult the Kaiser Permanente Oakland Proud pediatric gender clinic, where she could get further information and (gender affirming) “treatment.” Now I was the one feeling dizzy.
As I began educating myself on this issue, I discovered that this phenomenon—minors, most often teen girls, suddenly adopting trans identities—was becoming increasingly widespread. It even had a name: rapid onset gender dysphoria, or ROGD. Thankfully, after learning about the potential side-effects of blockers and hormones, my ex-husband and I managed to agree not to consent to any medical interventions for our daughter until she turned 18 and would then be able to make such decisions as an adult.
Over the past five years, my daughter’s identity has slowly evolved in ways that I see as positive. Our bond, however, has become strained, particularly since I began publicly voicing my concerns about what many term as “gender ideology.” Following my daughter’s 17th birthday family celebration, she sent me an email that evening stating she would be cutting off contact with me.
While this estrangement brought me sorrow, with my daughter living full-time with her father, it also gave me the space to be an advocate/activist in pushing back on gender identity ideology in the schools and the medical industry.
I decided to go undercover as a nonbinary patient to show my daughter what danger she might be putting herself in—by people who purport to have her health as their interest, but whose main interest is in medically “affirming” (i.e., transitioning) whoever walks through their door. I am at heart a mother protecting her child.
* * *
My daughter’s sudden decision to become a boy was heavily on my mind in early September of 2022, when mail from my Kaiser Permanente Davis Ob-Gyn reminded me of a routine cervical screening with “Recommended for people with a cervix ages 21 to 65.” I was told that the wording was chosen to be “inclusive” of transgender and “gender fluid” patients.
Throughout the whole 231-day process of my feigned gender transition, the Kaiser gender specialists were eager to serve me and give me what I wanted, which would all be covered by insurance as “medically necessary.” My emails were returned quickly, my appointments scheduled efficiently, and I never fell through the cracks. I was helped along every step of the way.
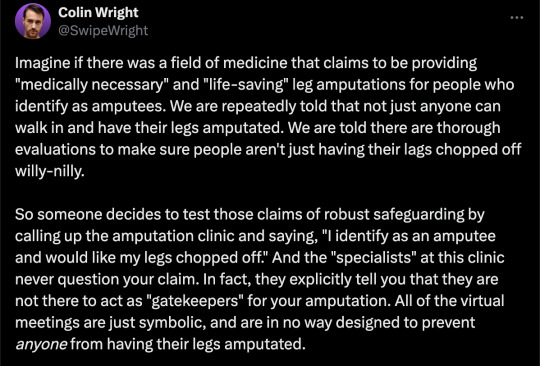
Despite gender activists and clinicians constantly claiming that obtaining hormones and surgeries is a long and complex process with plenty of safety checks in place, I was in full control at every checkpoint. I was able to self-diagnose, determine how strong a dose of testosterone I received and which surgeries I wanted to pursue, no matter how extreme and no matter how many glaring red flags I purposefully dropped. The medical workers I met repeatedly reminded me that they were not there to act as “gatekeepers.”
I was able to instantly change my medical records to reflect my new gender identity and pronouns. Despite never being diagnosed with gender dysphoria, I was able to obtain a prescription for testosterone and approval for a “gender-affirming” double mastectomy from my doctor. It took only three more months (90 days) to be approved for surgery to remove my uterus and have a fake penis constructed from the skin of my thigh or forearm. Therapy was never recommended.
Critics might dismiss my story as insignificant on the grounds that I am a 53-year-old woman with ample life experience who should be free to alter her body. However, this argument for adult bodily autonomy is a standard we apply to purely cosmetic procedures like breast implants, liposuction, and facelifts, not “medically necessary” and “lifesaving” treatments covered by health insurance. Or interventions that compromise health and introduce illness into an otherwise healthy body. And especially not for children.
My story, which I outline in much more detail below, should convince any half-rational person that gender medicine is not operating like any other field of medicine. Based on a radical concept of “gender identity,” this medical anomaly preys upon the body-image insecurities common among pubescent minors to bill health insurance companies for permanent cosmetic procedures that often leave their patients with permanently altered bodies, damaged endocrine systems, sexual dysfunction, and infertility.
* * *
Detailed Timeline of Events
On October 6, 2022, I responded to my Ob-Gyn’s email to tell her that, after some thought, I’d decided that maybe the label “cis woman” didn’t truly reflect who I was. After all, I did have some tomboyish tendencies. I told her I would like my records to be changed to reflect my newly realized “nonbinary” identity, and that my new pronouns were they/them. I also voiced my desire to be put in touch with an endocrinologist to discuss starting testosterone treatment.
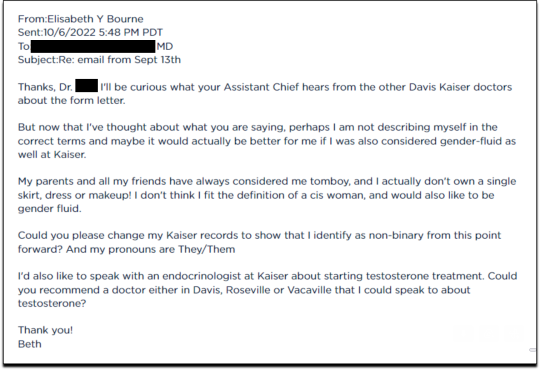
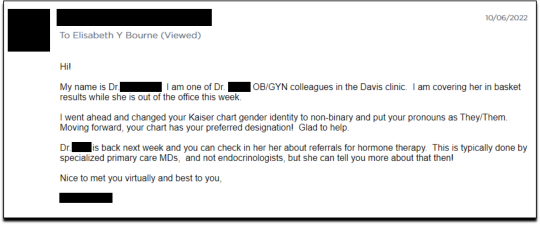
Fifteen minutes later I received an email from another Kaiser doctor informing me that my medical records had been changed, and that once my primary doctor returned to the office, I’d be able to speak with her about hormone therapy.
I responded the following day (October 7, 2022), thanking her for changing my records, and asking if she could connect me with someone who could help me make an appointment for “top surgery” (i.e., a cosmetic double mastectomy) because my chest binder was rather “uncomfortable after long days and playing tennis.”
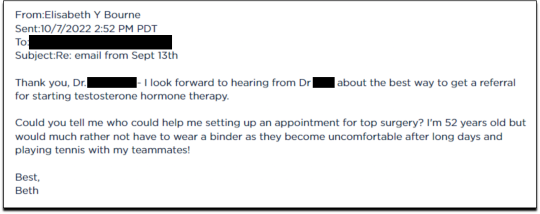
She told me to contact my primary care MD to “get things rolling,” and that there were likely to be “preliminary evaluations.”
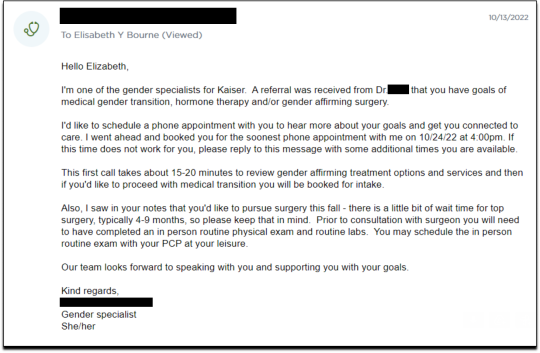
Six days after contacting my primary care MD for a referral, I received an email from one of Kaiser’s gender specialists asking me to schedule a phone appointment so she could better understand my goals for surgery, so that I could get “connected to care.” This call to review my “gender affirming treatment options and services” would take 15-20 minutes, after which I would be “booked for intake,” allowing me to proceed with medical transition.
This wasn’t an evaluation of whether surgical transition was appropriate, it was simply a meeting for me to tell them what I wanted so that they could provide it.
On October 18, I had my one and only in-person appointment in preparation for top surgery. I met in Davis with my primary care physician, Dr. Hong-wen Xue. The assessment was a 10-minute routine physical exam that included blood tests. Everything came back normal. Notably, there was not a single question about why I wanted top surgery or cross-sex hormones. Nor was there any discussion of the risks involved with these medical treatments.
The following week, on October 24, I had a phone appointment with Rachaell Wood, MFT, a gender specialist with Kaiser Sacramento. The call lasted 15 minutes and consisted of standard questions about potential drug use, domestic violence, guns in the house, and whether I experienced any suicidal thoughts. There were no questions from the gender specialist about my reasons for requesting a mastectomy or cross-sex hormones, or why I suddenly, at 52, decided I was “nonbinary.”
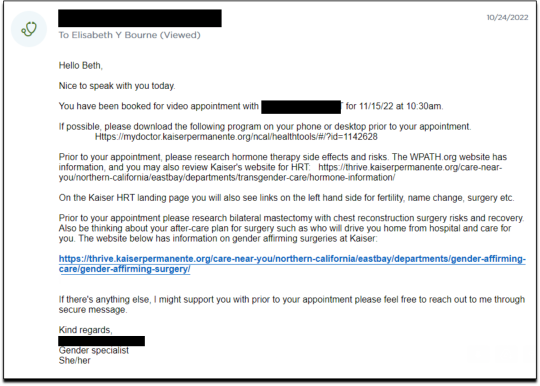
After the call, Kaiser emailed me instructions about how to prepare for my pre-surgery intake video appointment to evaluate my mental health, scheduled to take place on November 15. The email stated that prior to my appointment, I should research hormone risks on the WPATH website, and to “research bilateral mastectomy and chest reconstruction surgery risks and recovery” on Kaiser’s website.
I decided to request a “gender-affirming” double mastectomy and phalloplasty. Kaiser sent me a sample timeline for gender transition surgery preparation (see below) that you can use as a reference for the process. I also asked for a prescription for cross-sex hormones (testosterone) as needed and recommended by Kaiser.
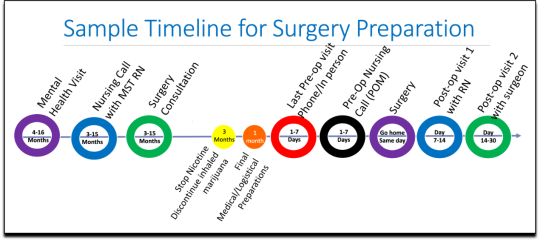
[ Source: Kaiser Permanente, Top Surgery - EXPLORING YOUR SURGICAL OPTIONS ]
Pre-Surgery Mental Health Video Appointment, Part I
This “Mental Health Visit” assessment was conducted over Zoom. The Kaiser gender specialist started with questions addressing my marital status, race, gender identity, and other demographics. She asked whether I was “thinking of any other surgeries, treatments in the future.” The list she read included “gender-affirming” hysterectomies, bottom surgeries such as metoidioplasty and phalloplasty, vocal coaching, support groups, and body contouring. “Anything else you might be interested in doing?” she asked. I said that I’d perhaps be interested in body contouring. I was also assured that all the procedures would be covered by insurance because they were considered “medically necessary.”
I dropped in several red flags regarding my mental health to see the reaction, but all were ignored. For instance, I revealed that I had PTSD. When the therapist asked me about whether I had experienced any “childhood trauma,” I explained that I grew up in Mexico City and had been groped several times and had also witnessed men masturbating in public and had been grabbed by men in subways and buses. “I was a young girl, so [I had] lots of experiences of sexual harassments, sexual assault, just the kind of stuff that happens when you are a girl growing up in a big city.” “So, you know,” I finished, “just the general feeling that you are unsafe, you know, in a female body.”
The therapist did not respond to my disclosure that trauma could be the cause of my dysphoria. Instead of viewing this trauma as potentially driving my desire to escape my female body through hormones and surgery, she asked whether there is anything “important that the surgery team should be aware of” regarding my “history of trauma,” such as whether I’d be comfortable with the surgeon examining and marking my chest prior to surgery.
When asked about whether I had had any “psychotic symptoms,” I told her that while I had had no such symptoms, my mother had a delusional nervous breakdown in her 50s because she had body dysmorphia and became convinced she had a growth on her neck that needed to be removed. I told her that my mother was then admitted to an inpatient hospital for severe depression. I asked her whether she ever sees patients with body dysmorphia and whether I could have potentially inherited that from my mother. She told me that psychosis was hereditary, but that it was “highly unlikely” that there was any connection between body dysmorphia and gender dysphoria.
I enthusiastically waved more mental health red flags, waiting to see if she would pick up on any of them.
I’m just wondering if my feelings, or perseverating, or feeling like these breasts make me really unhappy and I just don’t want them anymore!...I’m just not sure if that’s a similar feeling to body dysmorphia? How do you decide which one is gender dysphoria and general body dysmorphia, and just not liking something about your body? Feeling uncomfortable with your body?
And I did have an eating disorder all through college. I was a distance runner in college so I had bulimia and anorexia, you know. So I don’t know if that’s related to gender dysphoria?
The therapist replied, “I completely appreciate your concerns, but I am going to ask you questions about your chest, about your expectations. And then I’ll be able to give you an assessment.” She also said the main difference between my mom’s situation and mine was that my mom didn’t really have a growth on her neck, whereas it’s “confirmed” that I actually have “chest tissue.” Furthermore, she said that while “historically there has been all this pressure on patients to be like ‘Are you really, really sure you want hormones? Are you 100% sure?’ We are a little more relaxed.” She continued, “As long as you are aware of the risks and the side-effects, you can put your toe in the water. You can stop ‘T’ [testosterone], you can go back and do it again later! You can stop it! You can stop it! You know what I mean?”
Because we ran out of time, I scheduled a follow-up phone meeting on December 27, 2022 with a different gender specialist to complete my mental health assessment for top surgery.
Pre-Surgery Mental Health Video Appointment, Part II
During this meeting, Guneet Kaur, LCSW, another Kaiser gender specialist (she/her/they/them pronouns) told me that she regretted the “gatekeeping vibe” of the meeting but assured me that since I have been “doing the work,” her questions are essentially just a form of “emotional support” before talking with the medical providers.
She asked me about what I’d been “looking into as far as hormones.” I told her that I’d be interested in taking small doses of testosterone to counterbalance my female feelings to achieve “a feeling that’s kind of neutral.”
When she asked me about me “not feeling like I match on the outside what I feel on the inside,” I dropped more red flags, mentioning my aversion to wearing dresses and skirts.
I don’t own a single dress or a skirt and haven't in 20 years. I think for me it’s been just dressing the way that’s comfortable for me, which is just wearing, jeans and sweatshirts and I have a lot of flannel shirts and, and I wear boots all the time instead of other kinds of shoes. So I think it’s been nice being able to dress, especially because I work from home now most of the time that just a feeling of clothing being one of the ways that I can feel more non-binary in my everyday life.
She responded, “Like having control over what you wear and yeah. Kind of that feeling of just, yeah, this is who I am today. That’s awesome. Yeah.”
She then asked me to describe my dysphoria, and I told her that I didn’t like the “feeling of the female form and being chesty,” and that because I am going through menopause, I wanted to start taking testosterone to avoid “that feeling of being like this apple-shaped older woman.” “Good. Okay, great,” she responded, reminding me that only “top surgery,” not testosterone, would be able to solve my chest dysphoria. (Perhaps it was because all these meetings were online, they didn’t notice I’m actually fit and relatively slender at 5’-5” and 130 pounds, and not apple-shaped at all.)
She told me that we had to get through a few more questions related to my medical history before “we can move on to the fun stuff, which is testosterone and top surgery.”
The “fun stuff” consisted of a discussion about the physical and mood changes I could expect, and her asking me about the dose of testosterone I wanted to take and the kind of “top surgery” technique I’d prefer to achieve my “chest goals.” She told me that all or most of my consultations for surgeries and hormones would be virtual.
The gender specialist told me after the appointment, she would submit my referral to the Multi-Specialty Transitions Clinic (MST) team that oversees “gender expansive care.” They would follow up to schedule a “nursing call” with me to review my medical history, after which they’d schedule my appointment with a surgeon for a consultation. Her instructions for this consultation were to “tell them what you’re wanting for surgery and then they share with you their game plan.”
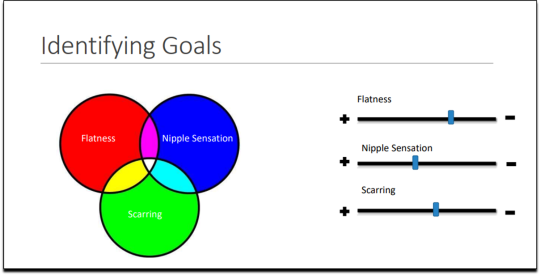
[ Decision-making slide to help me identify my goals for top surgery–flat chest, nipple sensation, or minimal scarring. Source: Kaiser Permanente, Top Surgery - EXPLORING YOUR SURGICAL OPTIONS ]
She told me that Kaiser has a team of plastic surgeons who “only work with trans and nonbinary patients because there’s just so much need for them.” She asked about my priorities for chest surgery, such as whether I value flatness over nipple sensation. I learned about double incision top surgery with nipple grafts, as well as “keyhole,” “donut,” “buttonhole,” and “Inverted-T” top surgeries.
By the end of the hour-long appointment, I had my surgery referral and was ready for my “nursing call” appointment.
Nursing call with Nurse Coordinator from the Transgender Surgery and Gender Pathways Clinic at Kaiser San Francisco
On January 19, 2023, I had my nursing call with the Nurse Coordinator. He first said that “the purpose of this call is just for us to go through your chart together and make sure everything’s as accurate as possible.” Once that was done, my referral would be sent to the surgeon for a consultation.
He asked me about potential allergies and recreational drug use, and verified that I was up to date on mammograms, pap smears, and colon cancer screenings, as well as vaccines for flu and COVID. I verified my surgical history as well as my current medications and dietary supplements.
He told me about a “top surgery class” available for patients where one of the Kaiser surgeons “presents and talks about surgical techniques and options within top surgery,” and includes a panel of patients who have had top surgery. I signed up for the February 8th class.
Within 10 minutes he told me that he had “sent a referral to the plastic surgery department at Kaiser Sacramento,” and that I should be hearing from them in the next week or two to schedule a consultation.
Appointment for Testosterone
On January 27, I had a 13-minute online appointment with a primary care doctor at Kaiser Davis to discuss testosterone. The doctor verified my name and preferred pronouns, and then directly asked: “So, what would you like to do? What kind of physical things are you looking for?”
I told her I wanted facial hair, a more muscular and less “curvy” physique, and to feel stronger and androgynous. She asked me when I wanted to start, and I told her in the next few months. She asked me if I was menopausal, whether I had ovaries and a uterus, although that information should have been on my chart.
The doctor said she wanted me to come in to get some labs so she could check my current estrogen, testosterone, and hemoglobin levels before starting hormones. Then “we'll set the ball in motion and you'll be going. We’ll see you full steam ahead in the direction you wanna go.”
That was it. I made an appointment and had my lab tests done on February 12. My labs came back on February 14, and the following day, after paying a $5 copay at the Kaiser pharmacy, I picked up my testosterone pump. That was easy!
Top Surgery Consultation
On the same day I received my labs, I had a Zoom surgery consultation with Karly Autumn-Kaplan, MD, Kaiser Sacramento plastic surgeon. This consultation was all about discussing my “goals” for surgery, not about whether surgery was needed or appropriate.
I told the surgeon that I wanted a “flatter, more androgynous appearance.” She asked me some questions to get a better idea of what that meant for me. She said that some patients want a “male chest,” but that others “want to look like nothing, like just straight up and down, sometimes not even nipples.” Others still wanted their chest to appear slightly feminine and only “slightly rounded.” I told her that I’d like my chest to have a “male appearance.”
“What are your thoughts about keeping your nipples?” she asked. “Are you interested in having nipples or would you like them removed?” I told her that I’d like to keep my nipples, but to make them “smaller in size.” She asked me if I’d like them moved to “the edge of the peck muscle” to achieve “a more male appearance.” I said yes.
I was asked to show my bare chest from the front and side, which I did. Then she asked me how important it was for me to keep my nipple sensation. I replied that it was important unless it would make recovery more difficult or there were other associated risks. She highlighted the problem with the free nipple graft, saying that removing the nipple to relocate it means “you're not gonna have sensation in that nipple and areola anymore.” However, some nipple sensation could be preserved by keeping it attached to “a little stalk of tissue” with “real nerves going to it,” but that would require leaving more tissue behind. I told her I’d go for the free nipple graft to achieve a flatter appearance. It was also suggested I could skip nipple reconstruction entirely and just get nipples “tattooed” directly onto my chest.
She told me I was “a good candidate for surgery,” and put me on the surgery wait list. She said that the wait time was between three and five months, but a cancellation could move me up to a sooner date. Also, if I wanted surgery as soon as possible, I could tell the surgery scheduler that I’d be willing to have any of the other three surgeons perform my mastectomy. Outpatient top surgery would cost me a copay of $100.
They contacted twice, in February and March, notifying me of cancellations. If I had accepted and shown up on those dates, they would have removed my breasts. This would have been less than five months from the time I first contacted Kaiser to inform them of my new “nonbinary” gender identity.
How Far Can I Go?
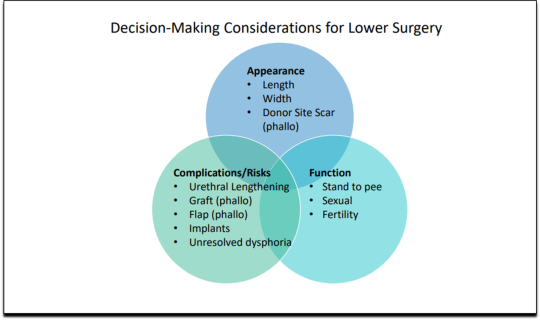
I decided to see how easy it would be for me to get approved for a phalloplasty. Known euphemistically as “bottom surgery,” phalloplasty is the surgical creation of an artificial penis, generally using tissue from the thigh or arm.
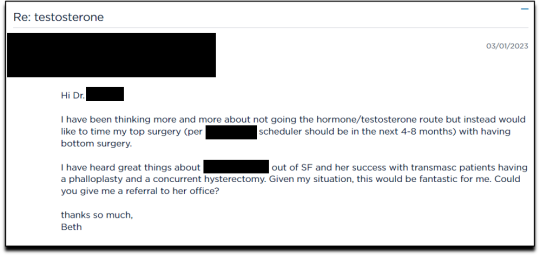
I sent an email on March 1, 2023, requesting to have a phalloplasty and concurrent hysterectomy scheduled alongside my mastectomy.
Two weeks later, on March 16th, I had a 16-minute phone call with a gender specialist to discuss my goals for bottom surgery and obtain my referral.
During the call, I explained to the specialist that I wasn’t sure about taking testosterone anymore because I was already quite athletic and muscular, and that taking testosterone didn’t make much sense to me. Instead, I wanted bottom surgery so that I wouldn’t feel like my “top” didn’t match my “bottom.” I told her:
But what I really wanted was to have bottom surgery. So this way when I have my top surgery, which sounds like it could be very soon, that I’ll be aligned, that I won’t have this sense of dysphoria with one part of my body and the other part feeling like it matched who I am. So yeah. So I just did a little bit more research into that. And I looked at the resources on the Kaiser page for the MST clinic and I think I know what I want, which is the hysterectomy and then at the same time or soon after to be able to have a phalloplasty.
I told her that I wanted to schedule the top and bottom surgery concurrently so that I wouldn’t have to take more time off work and it would save me trips to San Francisco or Oakland, or wherever I had to go for surgery.
None of this gave the gender specialist pause. After a brief conversation about some online resources to look over, she told me that she would “submit the referral now and we’ll get this ball rolling.”
Bottom surgery would cost me a copay of $200, which included a couple of days in the hospital for recovery.
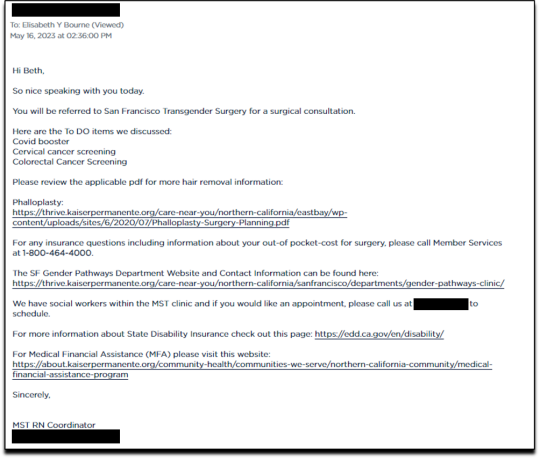
Phalloplasty Surgical Consultation with Nurse Coordinator
On May 16, 2023, I had a short surgical consultation with a nurse coordinator to go through my medical history. This was similar to the consultation for top surgery but included information about hair removal procedures for the skin on my “donor site” that would be fashioned into a makeshift penis. They also went over the procedures for determining which donor site—forearm or thigh—was more viable.
After only 15 minutes, she submitted my referral to the surgeon for another surgical consultation.
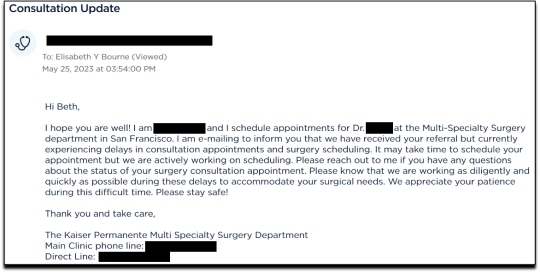
On May 25 I received an email from my phalloplasty surgeon’s scheduler, informing me that they have received my referral and are actively working on scheduling, but that they are experiencing delays.
I ended my investigation here once I had the referral for the top and bottom surgery. I never used my testosterone pump.
Final Thoughts
In fewer than 300 days, based on a set of superficial and shifting thoughts about my gender and my “embodiment goals” triggered by the mere mention of “gender” in a form letter from my primary care physician, and driven by what could only be described as minor discomforts, Kaiser Permanente’s esteemed “multi-disciplinary team” of “gender specialists” was willing, with enthusiasm—while ignoring mental health concerns, history of sexual trauma, and rapidly escalating surgical requests—to prescribe life-altering medications and perform surgeries to remove my breasts, uterus, and vagina, close my vaginal opening, and attempt a complex surgery with high failure and complication rates to create a functionless representation of a penis that destroys the integrity of my arm or thigh in the process.
This describes the supposedly meticulous, lengthy, and safety-focused process that a Kaiser patient must undergo to embark on a journey to medically alter their body. No clinician questioned my motivations. No one showed concern that I might be addressing a mental health issue through radical and irreversible interventions that wouldn’t address my amorphous problems. There were no discussions about how these treatments would impact my long-term health, romantic relationships, family, or sex life. I charted the course. The clinicians followed my lead without question. The guiding issue was what I wanted to look like.
No other medical field operates with this level of carelessness and disregard for patient health and welfare. No other medical field addresses issues of self-perception with surgery and labels it “medically necessary.” No other medical field is this disconnected from the reality of the patients it serves.
Kaiser has traded medicine for ideology. It’s far beyond time we stop the ruse of considering “gender-affirming” interventions as anything approaching medical care.
This isn’t the first time Kaiser Permanente has been in the news for completely disregarding medical safeguards in the name of “gender-affirming care.” As girls, Chloe Cole and Layla Jane became convinced that they were born in the wrong body and were actually boys on the inside. Doctors at Kaiser ignored their underlying conditions and instead prescribed testosterone and removed their breasts. Both Cole and Jane have since detransitioned and are currently suing Kaiser.
The fact that children and vulnerable adults are being exploited in this massive ideological experiment is not just tragic; it’s deeply disturbing, especially considering it has evolved into a billion-dollar industry.
I hope that by sharing my story, I can bring more focused scrutiny to the medical scandal unfolding not just at Kaiser but also at medical centers and hospitals across the Western world. These institutions have completely abandoned medical safeguards for patients who claim to be confused about their “gender,” and I aim to awaken more parents and assist them in protecting their children.
--
==
This is completely insane.
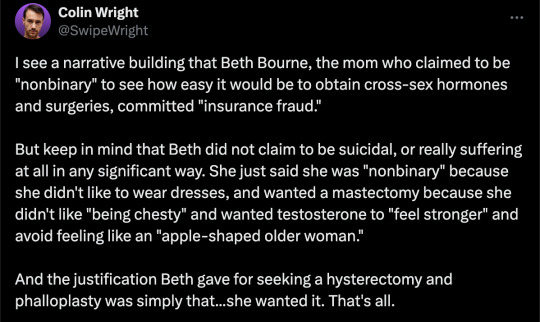
Apologists online are running around saying, but she didn't mean it, she was lying, she was pretending...
It doesn't matter.
Any kind of security, penetration or integrity test is insincere too. When security researchers compromise Microsoft's operating system or Google's browser or whatever, "but they didn't mean it" is not a defence to a discovered security flaw. It doesn't matter that the security researchers didn't plan to steal data or money or identities. The flaw in the system is there regardless.
It doesn't matter that it was insincere. Because the workers didn't know that. They never checked, never asked questions, never tested. They had been taught and instructed to never ask any questions. They did what they were supposed to. And the system failed spectacularly. Because that's what "gender affirming care" means.
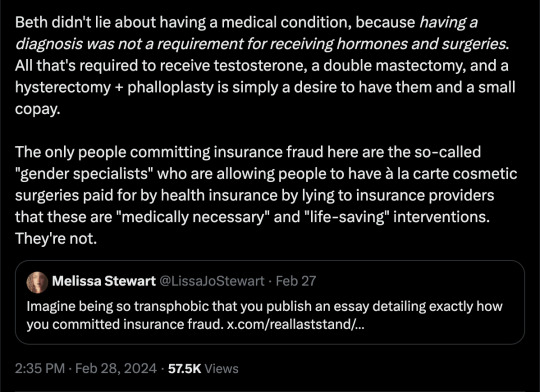
Additionally, the claim that Beth Bourne committed fraud is an outright lie. A patient cannot bill. They do not have the authority. The medical clinic is the only one that can bill, and they must supply a diagnosis and a medical necessity.
If they didn't diagnose her and just wrote down what she said, then they committed fraud. If they claim they did diagnose her, then they committed fraud, because the diagnosis they concocted was bogus. This, by the way, is actually going on. Clinics are reporting fake endocrine and other disorders to get blockers, hormones and other interventions. Jamie Reed and other whistleblowers have documented evidence of this. Beth Bourne is not responsible for what the clinic does. They have medical licenses and legal responsibility. Not her.
Additionally, anyone who actually read the article would know how she tested the system. She said things like, "I've always been not that feminine. So, maybe I get my boobs removed." And they said, "sure." Instead of saying, "wait, why do you think that?" Framing it as her lying is itself a lie. They violated their ethical obligations. That much is incontrovertible. And it's directly the result of "gender affirming care," where clinics and clinicians rubber-stamp anything deemed "trans" based entirely on ideological, not medical, grounds.
#Beth Bourne#undercover#undercover investigation#gender identity ideology#queer theory#nonbinary#non binary#top surgery#bottom surgery#double mastectomy#bilateral mastectomy#gender affirming care#gender affirming healthcare#gender affirmation#affirmation model#medical scandal#medical malpractice#medical corruption#religion is a mental illness
759 notes
·
View notes
Text
“The queer who is happily queer still encounters the world that is unhappy with queer love, but refuses to be made unhappy by that encounter. I have argued that the risk of promoting happy queers is that the unhappiness of this world can disappear from view. To be happily queer can also recognize that unhappiness; indeed to be happily queer can be to recognize the unhappiness that is concealed by the promotion of happy normativity. ”
(..)
“To be happily queer is to explore the unhappiness of what gets counted as normal. It is as if queers, by doing what they want, expose the unhappiness of having to sacrifice personal desires, in the perversity of their twists and turns, for the happiness of others”
Sara Ahmed, The Promise of Happiness
1K notes
·
View notes
Text
attention all students:
if your school offers a Queer Theory or LGBT+ History class, take it. find a way to sign up for it, ask a school counselor about it, research it - do whatever you can to take it. with all of these anti-queer bills and legislation coming out, learning our past is extremely important, now more than ever.
the QT class i took was majority oral history from my 70-something badass butch professor. she equipped me with priceless knowledge about all of the people that gave their lives for us to be even in public.
this is a plea to make an effort to preserve our history. no, im simply begging you. don't let them erase us again.
#i would take that class over and over and over again#lgbt#lgbtq#queer theory#gay#queer#college#class#student#history#important#politics#current events#don't say gay#me#mine#trans#transgender#USA#america#queer history
856 notes
·
View notes
Text
i find it so disingenuous that some people act like transmasculine people can't relate to transfem people.
transmasculine people, GNC cis women and butches, for *years*, have been writing about how they are seen as predatory in the women's restrooms because they 'look like men' or 'don't look woman enough' to be in there. i personally have experienced dirty looks and weird stares in the women's restroom as an openly butch person AFAB.
there are countless videos of cis women being removed from women's restrooms because they don't look 'woman enough' to be in there to take a leak. a video of a cis lesbian actually went viral for this.
there's a song by tribe 8, a lesbian queercore band, titled 'wrong bathroom' about these women not looking 'woman enough' to be able to use the women's restroom.
s. bear bergman has an essay titled 'tranny bladder', in hir book, 'butch is a noun', about how ze has been forced to be able to hold it instead of choosing to use the women's restroom because of how ze has been harassed in the women's restroom in the past over not looking quite 'woman enough', same for the men's restroom.
leslie feinberg wrote in hir book 'stone butch blues' about how the main character, jess, (butch) and her friend, ruth, (a trans woman), would declare that 'the world is our restroom' because of how they would rather use it on the side of the road than continue to be harassed in public restrooms about their presentations, assumed to be predatory.
like, do people just think that transmasculine people are not seen as predatory at all?
trans women are hypervisible and that definitely leads to them being labeled as predatory in a much more visible manner, but just because you don't see it, just because it may not be reported on as much or go viral, does not mean that transmasculine people aren't seen as predatory, and the idea that we can't be seen as predatory or that we have some sort of special privilege that means we're somehow not seen as predatory by society is, frankly, dangerous, especially for younger transmasculine people, who are going to experience a pretty rude awakening in the real world when they get questioned and harassed or even removed for not looking 'female enough' to use the women's restroom.
#txt#anti-transmasculine transphobia#transandrophobia#transmisandry#only reason i use those two terms#is for visibility#gender theory#transgender theory#queer theory#gender studies#trans#transgender#transsexual#transmasculine#transfeminine#transmasc#transfem#transfemme#mtf#ftm#discourse#lgbt discourse#queer discourse
1K notes
·
View notes
Text
Butch/Femme history and culture introduction (written by a femme lesbian, deeply in love with being so)
💖Ideal for people immersing themselves in lesbian culture for the first time
🤍This post will contain brief summarising information about butch/femme culture and history as well as an introductory resource list for continuing your learning journey.
🧡It is by no means exhaustive and is intended as a very basic and simplified introduction that people can and should easily build on. Please try to keep this intention in mind before telling me i have neglected something!
⚠️ Disclaimer - this post is admittedly very centred on butch/femme history of the US and western culture in the 1900s. If there is a different culture or time that you’d be interested to learn more about, I would be overjoyed to research it so please let me know! Lesbianism has existed everywhere in every time and the cultural variation of this is beautiful and SO important. I do not want to neglect that but cannot fit it all in this brief introduction post.
“Whether reclaiming femininity from the male gaze or rejecting feminine gender norms by embracing butch, the subculture is intrinsically radical: it empowers lesbians to renounce patriarchal standards of beauty.” - Megan Christopher
What is butch/femme?
butch/femme is a lesbian subculture with a deep and rich history and culture. It goes far beyond masculine and feminine aesthetics and informs lesbian identity and dynamics. Butch/femme culture is a crucial part of LGBTQ+ history and culture as a whole.
It has existed for a very long time but it is very important to know that not all lesbians are butch/femme. In fact, most lesbians will not identify with either label and that is completely okay! You will see some lesbians describe themselves as butch4butch or femme4femme.
Traditionally, there is nothing in between butch/femme and to suggest otherwise negates the rich significance of the identities. Some people suggest it is a spectrum with “futch” in the middle. This is however not the case and the significance of this will become clear as we delve further into the importance of butch/femme identities to queer culture and history. Crucially too, straight women cannot be butch/femme
Aren’t butch/femme just replicating traditional heterosexual gender roles?
Absolutely not! In fact, they outwardly challenge them.
Gender and sex are constructs. A lot of lesbians find that butch/femme are gender identities in of themselves (myself included)
Instead, butch/femme are identities that encapsulate a particular “performance” of gender. The attributes of these may seem “masculine” or “feminine” but this is only because of the strict gender binary our society ascribes to gender performance.
Judith Butler, in their book Gender Trouble, notes that a lot of lesbians in general have a complex relationship to gender. This is because our binary perception of womanhood is constructed on the basis that “male” is default and “female” is the only sexed other. Because lesbianism is the only identity that totally de-centres men, a lot of lesbians (regardless of being butch, femme or neither) will not feel like they are conventionally “women”.
A lot of the time, butch/femme roles were and still are a source of safety and solace
Butch
Butch refers to masculinity in any number of ways
Butches typically and historically face high levels of discrimination and harassment for their gender non conformity.
A very important butch text is Stone Butch Blues, written by Leslie Feinberg
In the book, Feinberg discusses the importance of working-class identities to butchness.
Some butches are transmasculine. This doesn’t make them less of a lesbian, as long as they have ties to butchness and lesbianism.
Stone butches are lesbians who do not like to be touched (or “receive”) during sex
Femme
Femmes are lesbians who present more “femininely”.
Femmes do not necessarily conform to society’s perception of womanhood. Many will have complex relationships to gender identity or will present as hyper-feminine.
Hyper-femininity is an exaggerated performance of womanhood where aspects of dress, character and/or mannerisms of femininity may be heightened.
This is why a lot of the time lesbians can still “clock” (or recognise) femmes as being gay. Straight women tend to feel put off by the level of femininity common with hyper-feminine femmes.
History
In western culture, butch/femme culture existed underground or secret up until the mid 20th century. We can assume however that butch/femme dynamics have existed for a long time.
In the early 1900s, butch/femme dynamics were confined to underground gay bars.
In this case, femmes were often considered in a position of privilege as they were “straight passing” and could only be recognisably lesbian when accompanied by a butch.
Femmes will often assert sexuality through their femininity.
In the 1940s, butch/femme dynamics were extremely important and a thriving part of lesbian culture.
Women were allowed to enter bars without men.
In the US, butches would have to dress femininely in order to hold employment and avoid harassment and assault based on their preferred gender non-conformity.
Butches dressed in a way that was accepted by society, while still presenting as more masculine than the norm. Alix Genter writes that "butches wore long, pleated skirts with their man-tailored shirts, sometimes with a vest or coat on top"
In the 1950s, many butches refused to live these double lives. Their full-time masculine presentation made it difficult for them to work so they were often employed in factories or as taxi drivers. (hence the importance of working-class solidarity with butches)
Increased lesbian visibility and a strong anti-gay political stance at the time of McCarthyism led to increased attacks on queer women and resulted in a particularly defiant gay bar culture.
Butches are therefore extremely important in our fight for LGBTQ+ rights. It was butches and trans women who were known for fighting back for our rights and visibility.
In the 1970s, particular sentiments of lesbian separatist feminism declared masculinity and butchness was harmful to women. This led to the popularisation of more androgynous fashion amongst lesbians including boots, jeans and flannels. This movement weakened butch identifiers and is known for alienating lesbians of colour and working class lesbians.
Lesbian separatism is essentially the idea that lesbians should exist separate to men and heterosexual women. That is why some theorists believed performances of masculinity were harmful (while others did not believe this and it is obviously not true)
Introductory reading list (online articles that are short and accessible)
how butch/femme subcultures allow gay women to thrive by Megan Christopher for VICE: https://www.vice.com/en/article/wjwzqx/how-butch-femme-subcultures-allow-gay-women-to-thrive
A good introduction to the radical history and importance of butch/femme identities.
The Lesbians That Founded The Gay Village And The Mafia Alliance They Made For Protection by Diana Robertson: https://www.huffpost.com/entry/the-lesbians-that-founded-the-gay-village-and-the-mafia_b_5941d7a1e4b0d99b4c921126
Really helpful history!
No Matter What’s Gendertrending, the Butch is Here To Stay by Jack Halberstam
https://web.archive.org/web/20180907141513/https://www.afterellen.com/tv/443117-no-matter-whats-gendertrending-the-butch-is-here-to-stay
I don’t like the suggestion of the title but the article itself has good information. Jack Halberstam is an important queer theorist. I also recommend his writings on queer failure. This article has some generally good direction about butchness, especially in modern media. “Butch is always a misnomer; masculine but not male, female but not feminine, the term serves as a placeholder for the unassimilable, for that which remains indefinable or unspeakable within the many identifications that we make and that we claim.”
Key books for a deeper understanding (and their pros and cons)
The Persistent Desire: A Femme–Butch Reader by Joan Nestle
Gender Trouble by Judith Butler (one of my favourite books of all time. Really difficult to get through but very worthwhile and completely changed the way I understand sex and gender)
Stone Butch Blues by Leslie Feinberg (an incredibly important lesbian text. Can be very difficult to get through, especially emotionally. Please make sure to check triggers before reading)
Dagger: On Butch Women by Lily Burana
#lgbtq#lgbt#lgbtqai#gay#lesbian#queer#sapphic#wlw#transgender#mlm#femme#butch#butch and femme#butch4femme#femme4butch#femme4femme#butch4butch#queer history#lesbian history#queer theory
482 notes
·
View notes
Last Seen Blogs

chetnasoni
Untitled


borderlinelifer
"Tell Him, Theres Too Much Beauty To Quit."

clothesonfilm
Clothes on Film

baysiderelationships-blog1
Bayside Relationships & Counselling